
Future Perspectives on the Treatment of Achondroplasia
Treatment options for individuals with achondroplasia (ACH) are currently inexistent. Only surgical corrective approaches are possible, and also limb lengthening is an option which can pose several complications. [1]
|
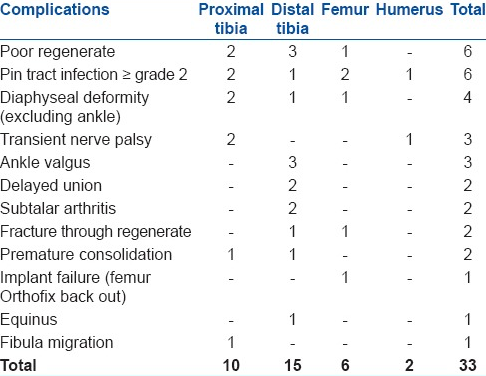
Fig. 1. Distribution of complications encountered during lengthening procedure, in Limb lengthening in achondroplasia. Sanjay K Chilbule, Vivek Dutt, Vrisha Madhuri. Indian J Orthop. 2016 Jul-Aug; 50(4): 397–405. |
Today, the management and treatment of ACH are major challenges for many centers involved in research concerning rare skeletal disorders, and we are witnessing the advent (and advancement) of several clinical trials in children with ACH. These developments were possible because of successful preclinical studies with mice that led to new insights into the FGFR3 mechanism of action and opened the door for new strategies and therapeutic approaches in humans. [2]
|
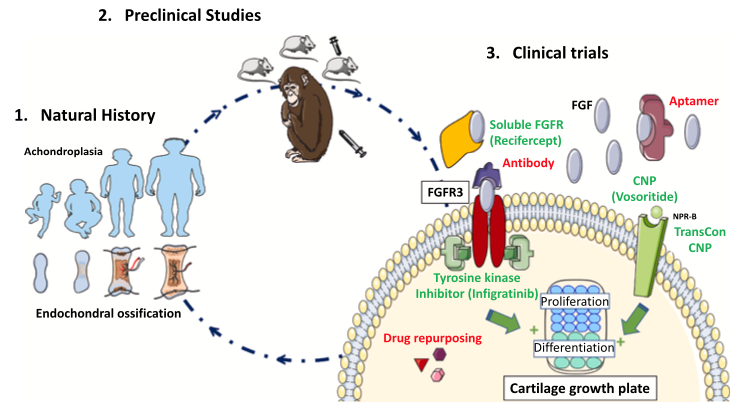
Fig. 2. Drug development process for achondroplasia. Legeai-Mallet, L., & Savarirayan, R. (2020). |
Such therapeutic approaches are currently under clinical trials to evaluate safety, efficacy, and pharmacokinetics, and include: Ribomic’s fibroblast growth factor aptamer (APT-F2P/RBM 007), Pfizer’s soluble FGFR3 decoy receptor (TA-46/recifercept), Rainier’s anti-FGFR3 antibody (B-701/vofatamab), QED’s Tyrosine kinase inhibitor (BGJ398/infigratinib), Nagoya University's drug repurposing of meclozine, and drugs that modulate growth plate homeostasis, which include BioMarin’s CNP analog (BMN111/vosoritide) and Ascendis’ TransCon CNP (more information can be found here). [2]
The main challenge of these studies resides on finding the balance between harm and benefit treating ACH in growing individuals. To find the right therapy, at the right time and dose, a comprehensive study is essential. One that combines natural history, preclinical data and clinical trials to better understand this condition and to facilitate strategies and precision therapeutics that allow a sensible approach to the potential harms that come with pediatric drug treatment (as the patient's organs are still in development).
Recent results of phase 2 and phase 3 clinical trials of CNP therapy in children with ACH have showed that major milestones have been achieved. [3, 4] Yet, other therapeutic options are emerging, and there are open possibilities for combination or sequential, age-oriented, precision therapy in the future.
Another important step still to be taken will be treating adults with ACH. Here, the goal is to ease complications such as spinal stenosis, intervertebral disc disease, bone homeostasis, and other non-skeletal complications that might affect life span (i.e., cardiovascular). [2]
There is hope that these new therapies will give better, non-surgical options for individuals with ACH to optimize their health and well-being and minimize the medical impacts of their condition.
References
1. Sanjay K Chilbule, Vivek Dutt, Vrisha Madhuri. Limb lengthening in achondroplasia in Indian J Orthop. 2016 Jul-Aug; 50(4): 397–405.
2. Legeai-Mallet, L., & Savarirayan, R. (2020). Novel therapeutic approaches for the treatment of achondroplasia. Bone, 141, 115579. https://doi.org/10.1016/j.bone.2020.115579
3. R. Savarirayan, et al, C-type natriuretic peptide analogue therapy in children with achondroplasia, N. Engl. J. Med. 381 (1) (2019) 25–35.
4. R. Savarirayan, et al, Once-daily, subcutaneous vosoritide therapy in children with achon- droplasia: a randomised, double-blind, phase 3, placebo-controlled, multicentre trial, Lancet 396 (2020) 684–692.

