
The cranial "domino" in achondroplasia
Excerpt from the book:
"Human achondroplasia, a multidisciplinary approach"
Benedetto Nicoletti, Elio Ascani, Victor A. McKusick, Shona C. Dryburgh, Springer Science & Business Media, 06/12/2012 - 514 pages
"The craniofacies in achondroplasia is typical and produced by decrease in the growth of the endochondrial bone growth at the base of the skull. Interestingly, Cohen et al. have shown that not all the cartilage bones at the base of the skull are involved to the same degree.
There are five practical problems which occur because of the midface constriction. The first is that children have relative tongue thrust. This may lead to feeding and respiratory problems in the newborn period. The respiratory problems are to be dealt with in another section, but practically speaking cleft palate nipples have been used with success for the feeding problems related to tongue thrust. If profuse sweating occurs during feeding, blood oxygenation should be checked.
Because the base of the skull is relatively small, the Eustachian tubes are short and small. In addition, because children with achondroplasia are relatively hypotonic, they may spend too much of their first year lying in bed. This combination leads to the marked increase in otitis media and the accumulation of fluid in the middle ear seen in childhood in achondroplasia.
Our study of adults with achondroplasia indicated that fully 75% have hearing problems. Glass et al. have shown many individuals with achondroplasia have neurosensory hearing loss as well. This is an area which requires careful observation in the young child and vigorous therapy to avoid chronic fluid fills the middle ear chronically in childhood. In addition, without good auditory input, speech development is usually delayed.
Delayed speech in achondroplasia may also occur because of the shape and relationship of the mouth and tongue. The relatively large mandible compared with the underdeveloped maxilla often gives relative tongue thrust. Speech in achondroplasia is often delayed and may require speech therapy. As much obvious, adequate hearing and speech are necessary for normal social interactions in young children as well as later in life.
The relatively larger mandible and small maxilla also lead to dental malocclusion. The orthodontic area requires careful monitoring in childhood. In general at about five to six years of age, a careful orthodontic evaluation should be done and a plan of overall therapy worked out. The new dental expanders may work for enlarging the maxilla area in achondroplasia. The more traditional orthodontic therapy in achondroplasia was to pull teeth in the mandible in order to keep it from growing as large as it normally would, thus making it more proportionate with the small maxilla.
The craniofacial abnormalities lead inevitably to a mild to moderate cosmetic problem of midface hypoplasia for most individuals with achondroplasia. Cosmetic therapy or surgery are usually not considered for this problem; however, a whole range of other problems from dental to respiratory may relate to the underdevelopment of the midface."
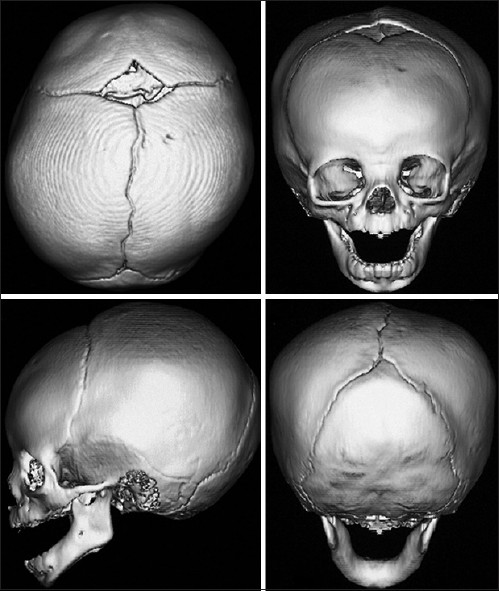
| The sutures in a normal infant. "Craniosynostosis", Ramesh Kumar Sharma. |
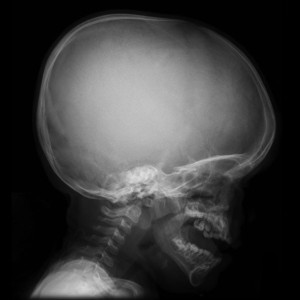
These two images are used to compare the size of the mandible and maxilla and skull base in children with similar ages, the first is a healthy child and the second has achondroplasia.
Although the author referred the age between 5 to 6 years old for the first orthodontic evaluations, they can be done earlier, around 3 years old. Speech therapist and orthodontist are essential for the evaluation and therapeutics of a child with achondroplasia during early childhood.


{kind=link}