
Limb Lengthening And Deformity Correction Surgery
What is limb lengthening surgery and what is its purpose?
Limb lengthening surgery is a form of distraction osteogenesis (bone lengthening surgery). It consists of cutting a section of a bone of the arms or legs and gradually pulling the two resulting pieces apart using a piece of equipment called a fixator. New bone (called regenerate) will form in that gap, effectively making the bone longer [1]. Lengthening of the lower limbs usually involves application of a fixator to both the tibia and the femur, while upper limb lengthening is usually done to the humerus [2].
It can be performed to:
- Correct deformities, such as genu varus;
- Increase stature.
The corrective technique used for deformity correction depends on the deformity and on any underlying conditions. It can consist on the insertion of a nail in the growth plate, halting growth on one side of the bone (called an epiphysiodesis), it can be an osteotomy, where the surgeon cuts a piece of the bone and uses fixators to correct the deformity, or it can be just a distraction, where fixators are fixed to the bone and gradually pull the joints into their proper position.
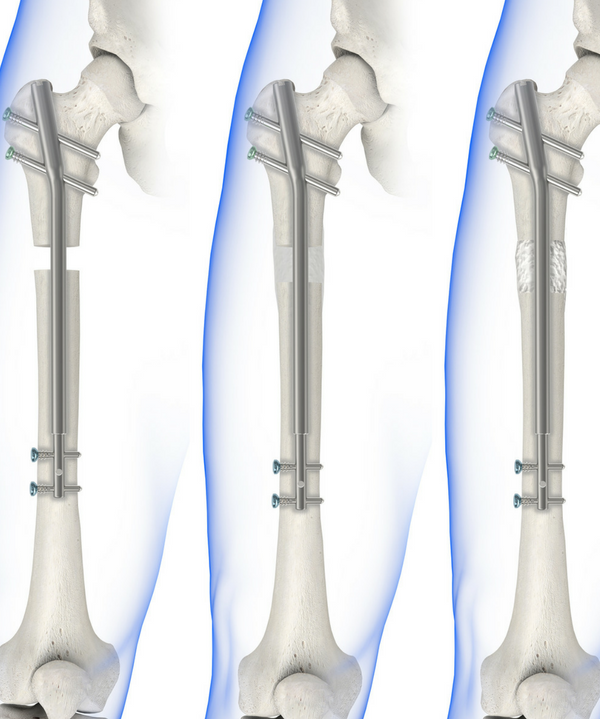
Fixators can be internal or external and can be used in conjunction. There are also several different internal and external aparatuses for limb lengthening and deformity correction. For example, the most known fixator is Ilizarov's circular external fixator, but there's also the PRECICE internal fixator, which is a long rod that is inserted directly into the bone and controlled externally using powerful magnets (animation on how it is implanted here). The PRECICE internal fixator can't be used on the humerus.
 |
 |
|
Ilizarov's external fixator (left) and representation of the PRECICE internal fixator (right). Credits: Ilizarov: https://ourorthopaedics.blogspot.com; PRECISE: Wikimedia Commons. |
What limb deformities can be corrected?
Genu varus can be corrected at the same time that tibial lengthening is performed, and coxa vara and fixed flexion of the hip can be corrected, which, in turn, will reduce the excessive lumbar lordosis [3, 4].
And how much height is possible to be gained?
The possible height gain varies according to each author. Some authors, like Dr. Paley, report that lengthening up to 40 cm of the lower extremities is possible without complications (more than 50% of the bone length in 3 or 4 sessions [3, 4]). Others defend that no more than 50% of the bone's total length should be increased (no more than about 10 cm), due to growth rate disturbances after limb lengthening [4, 5].
How long does the treatment take?
Time spent with a fixator can vary, and to achieve more than 10cm of extra height, more than one treatment is needed (usually at least 2 are performed). Typically, time spent with a fixator per treatment is about 1 month per lengthened centimeter in children and 1.5 months (or more) per centimeter for adults, divided between the two phases of limb lengthening [6, 7]:
Distraction phase (or lengthening phase)
This is the actual lengthening phase, where the two pieces of the bone are distracted from each other. The rate of distraction may vary, but it can go up to 1mm per day. As the bones lengthen the muscles will be pulled tighter and range-of-motion will decrease, physical therapy is a necessary component of recovery and a successful lengthening (without loss of function), and starts right after the person's discharged from the hospital [6].
Consolidation phase
When no more adjustments to the fixator are made, allowing the bone to heal with the new length. Physical therapy continues during this phase and after it finishes [6].
What complications can occur?
There are complications related to the surgery itself:
- Premature consolidation;
- Delayed and failed bone formation;
- Nerve stretch injury (when nerves are stretched beyond their limit);
- Joint and muscle contractures;
- Joint subluxation [8];
- Foot deformities [9].
And there are complications related to the devices themselves:
External fixators have high rates of complications related to the device itself, such as pin tract infections (infections around the fixation pins), joint and muscle stiffness, neurovascular injuries and large scars caused by the pins [8, 10].
Internal fixators don't cause most of the complications seen in external fixators, but they can need a minimum bone diameter to be applied, and can break and malfunction [2, 6], and the whole process must be very well planned, since postoperative changes (besides distraction rate) can't be made [10]. However, some internal fixators allow for the device to be shortened if there's need. Also, some internal fixators, such as PRECICE can't be used on the upper limbs.
How long does it take to recover?
As mentioned above, the recovery period is about a month per centimeter, which means that recovery time per treatment is about 5 to 7 months [3] added to the time it takes for the bone to regain normal strength (2 years) [9]. In total it takes about 2.5 years.
At what age can limb lengthening surgery be performed?
This point is also debatable. Most authors recommend starting at about age 8, but at this age it is generally considered that the child does not to have the capacity to decide what he/she really wants regarding this subject [4, 12]. In several European countries, the limb lengthening process is started when the child reaches 12 years old.
Sources
- Spiegelberg B, Parratt T, Dheerendra S, Khan W, Jennings R, Marsh D. Ilizarov principles of deformity correction. Annals of The Royal College of Surgeons of England. 2010;92(2):101-105. doi:10.1308/003588410X12518836439326.
- Paley, D. Four Segment Lengthening. Achondroplasia 2014 [cited 2017 30/11].
- Paley, D. Treatment Strategies. Achondroplasia 2014 [cited 2017 29/11].
- Donaldson J, Aftab S, Bradish C. Achondroplasia and limb lengthening: Results in a UK cohort and review of the literature. Journal of Orthopaedics. 2015;12(1):31-34. doi:10.1016/j.jor.2015.01.001.
- Song, S.H., et al., Growth disturbance after lengthening of the lower limb and quantitative assessment of physeal closure in skeletally immature patients with achondroplasia. J Bone Joint Surg Br, 2012. 94(4): p. 556-63.
- Paley, D. How Does Limb Lengthening & Deformity Correction Work? Limb Lengthening & Deformity Correction 2014 [cited 2017 29/11].
- Chilbule SK, Dutt V, Madhuri V. Limb lengthening in achondroplasia. Indian Journal of Orthopaedics. 2016;50(4):397-405. doi:10.4103/0019-5413.185604.
- Paley, D., PRECICE intramedullary limb lengthening system. Expert Rev Med Devices, 2015. 12(3): p. 231-49.
- Park, K.W., et al., Limb Lengthening in Patients with Achondroplasia. Yonsei Med J, 2015. 56(6): p. 1656-62.
- Thaller, P.H., et al., Limb lengthening with fully implantable magnetically actuated mechanical nails (PHENIX((R)))-preliminary results. Injury, 2014. 45 Suppl 1: p. S60-5.
- Wiebking U, Liodakis E, Kenawey M, Krettek C. Limb Lengthening Using the PRECICETM Nail System: Complications and Results. Archives of Trauma Research. 2016;5(4):e36273. doi:10.5812/atr.36273.
- Schiedel, F. and R. Rodl, Lower limb lengthening in patients with disproportionate short stature with achondroplasia: a systematic review of the last 20 years. Disabil Rehabil, 2012. 34(12): p. 982-7.

