
A silent risk in limb lengthening surgery - Fat embolism
Adipocytes, also known as fat cells, are the cells that primarily compose adipose tissue, specialized in storing energy as fat.
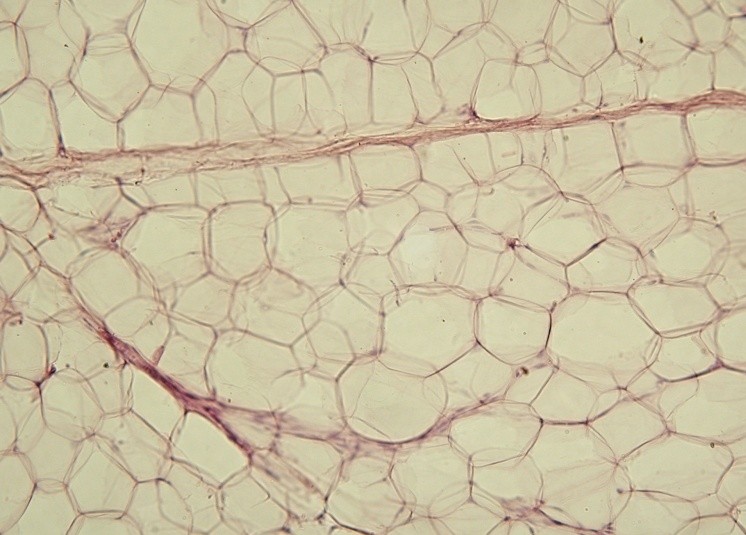
| "Yellow adipose tissue in paraffin section - lipids washed out". Licensed under CC BY-SA 3.0 via Wikimedia Commons |
Bone marrow is the flexible tissue in the interior of long bones. The two types of bone marrow are "red marrow", which consists mainly of hematopoietic tissue, that originates blood cells: erythroid cells (red blood cells) , lymphocytes (white blood cells) and myelocytes (as platelets), and "yellow marrow", which is mainly made up of fat cells.
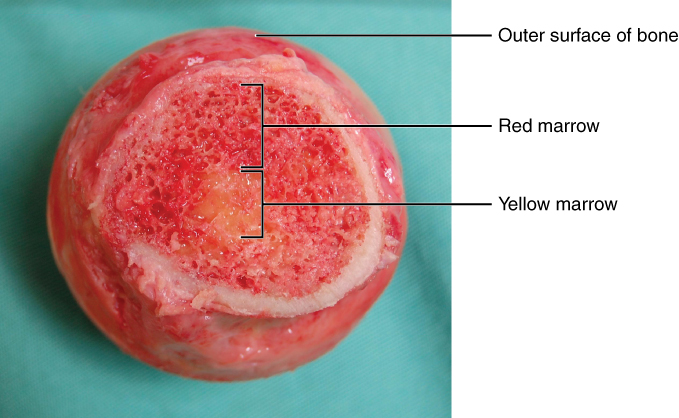
| A femoral head with a cortex of cortical bone and medulla of trabecular bone. Both red bone marrow and a central focus of yellow bone marrow are visible. "619 Red and Yellow Bone Marrow" by OpenStax College - Anatomy & Physiology, Connexions Web site |
"Fat embolism syndrome (FES) was first described by Von Bergmann in 1873 in a patient with a fractured femur. While fat within the circulation (fat embolism) is relatively common following long-bone fracture, the clinical pattern of symptoms that make up FES is less so, occurring in 1% to 3% of isolated long-bone fractures and 5% to 10% of patients with multiple skeletal trauma." (Excerpt from the American Journal of Orthopedics)
"Fat embolism syndrome (FES) is rare in pediatric patients; it is approximately 100 times less likely to develop in children and adolescents than in adults. The mortality rate for FES in children ranges from 1% to 15%, somewhat lower than that in adults (10%-20%). FES most often occurs after fractures of the long-bones, primarily the femur and pelvis. The development of FES after intramedullary nailing of long-bones in adults is well-described, with identified risk factors of advanced age, polytrauma, prolonged immobilization, and male sex. To our knowledge, there have been no documented cases of FES after isolated closed tibial shaft fractures but before operative treatment." (Excerpt from the case report "Fat Embolism Syndrome in an Adolescent Before Surgical Treatment of an Isolated Closed Tibial Shaft Fracture" R. Sawyer, et al, Dec 2012).
In a very conclusive article:

