This web site uses cookies. Do you accept the use of external cookies? YesNoKnow morex
Survey about achondroplasia
We have designed a questionnaire with the purpose to better know the population connected to achondroplasia.
The questionnaire is optional and anonymous. The data obtained will be used for statistical purposes and to better understand the natural history of achondroplasia. Please consider answering.
If you would like to take the survey later, you can click on the link at the top "Register at BA"
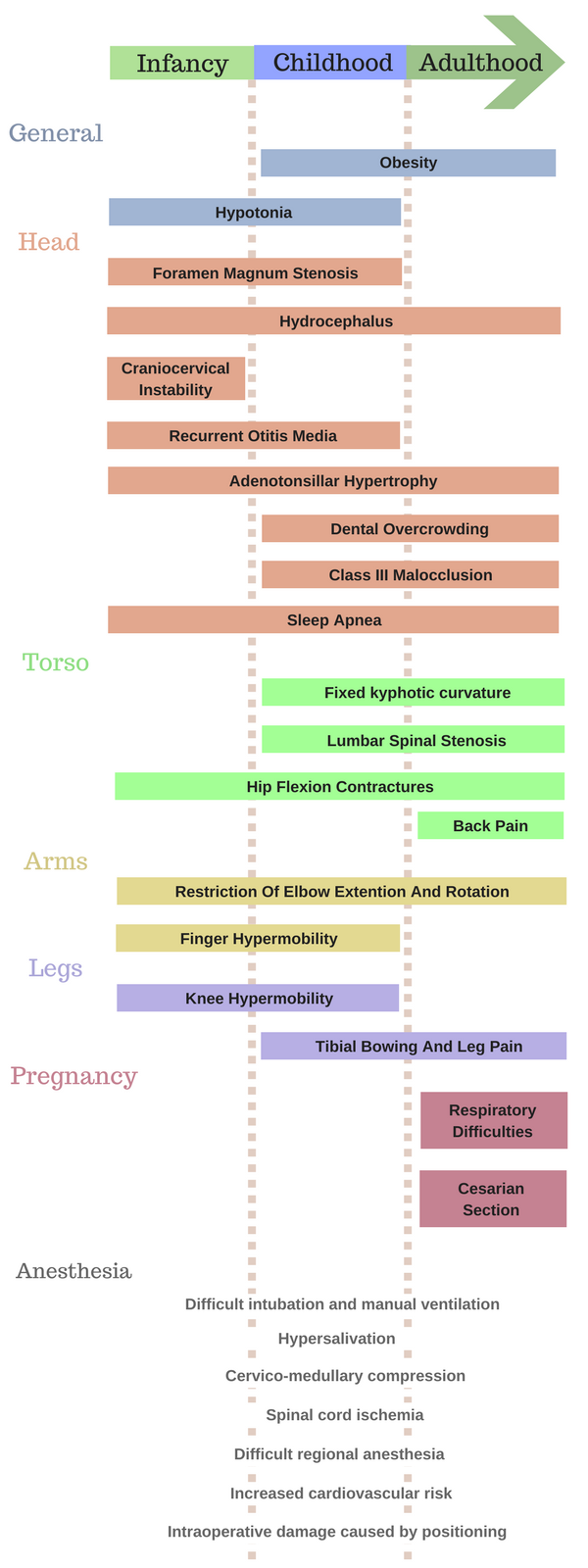
Obesity in late childhood can contribute to other complications such as hyperlordosis, genu varum, obstructive sleep apnea and spinal stenosis [1];
Hypotonia possibly caused by hyperextension injuries during delivery or by spinal cord constriction [1].
Head:
Compression at the foramen magnum (affects 5 to 10% of children) can lead to central sleep apnea, respiratory abnormalities, myelopathy (neurologic deficit related to the spinal cord), hydrocephalus and sudden infant death. Cervicomedullary decompression is necessary for up to 28% of children by 4 years of age - careful assessment of craniocervical risk should be made for every infant with achondroplasia, which includes: neurological history and examination, neuroimaging and polysomnography. Continuous management of this complication is still debatable. Some clinicians defend that routine cranial imaging should be performed routinely, while others suggest that investigation should only be performed if suggestive clinical evidence is present. Surgical cervicomedullary decompression may be needed [1-3];
Hydrocephalus (6% of children [2]), caused by restricted craniocervical junction. Referral to a neurosurgeon is necessary if there is rapid change of head circumference/size or if the head circumference is above the 95th percentile. Since it is more likely to develop during the first two years of life, occipital-frontal circumference (OFC) should be monitored frequently for the first year [1, 4];
Up to 89% of children suffer at least one episode of otitis before their second year of age and recurrent otitis media that can lead to hearing loss was observed in 25% of children – it is recommended to treat it aggressively, with adenotonsillectomy and insertion of grommets (ventilation tubes) to prevent hearing loss [1];
Dental overcrowding - regular dental reviews are recommended [2];
Class 3 malocclusion (underbite) - all children should be evaluated for possible orthodontic needs by age 6 [6];
Sleep apnea (affects up to 75% of children). Continuous positive airway pressure may be needed. If associated with gastroesophageal reflux and hypoglossal canal stenosis requires complex management, which may include foramen magnum decompression. When associated with hydrocephalus and muscular upper airways obstruction, sleep apnea responds well to treatment of hydrocephalus [1, 2].
Torso:
Neurological signs (manifestations of spinal stenosis) can be recognized by numbness or weakness in the legs after walking that occur associated with bladder or bowel dysfunction [2]. Claudication and hyperreflexia and are shown by 10% of children by 10 years of age - it is recommended to avoid premature sitting and baby wraps or swings which do not have head support, and to stretch the hip while stabilizing the lumbar spine [1]. Decompressive laminectomy is rarely indicated in children [2];
Hip contractures that contribute to lordosis (the deep curvature of the lower back), back pain and muscle fatigue - certain exercises can reduce lordosis and hip-flexion contractures [1, 4];
Restriction of elbow rotation and full extention [7]. This reduces the arm span, the ability to reach objects and do private hygiene;
Joint hypermobility and joint contractures in specific joints (finger hypermobility and elbow contractures) [1, 2];
Venous access is more difficult due to laxity and excess of skin and subcutaneous tissue [8].
Legs:
Knee hypermobility and instability of the soft tissues surrounding the knee. It may lead to difficulty walking, chronic pain, or a thrust of the knee, for which it’s recommended to consult an orthopaedist [1, 2, 4];
Leg pain associated with tibial bowing present in 40% of children and with rapid progression between 3-4 and 6-7 years [1]. Individuals that show leg pain or altered gait may need corrective surgery [4];